We need a plan to move the country forward and need one now. I am tired of hearing arguments based on “breaking news,” supercomputer modeling or economic formulas. I am therefore proposing this simple way to allow most people to lead normal lives while avoiding most (94%) deaths from COVID-19.

There is now a significant experience with COVID–19 infection, and we know that almost everyone without health issues and under the age of 60 does not get seriously ill from the virus. In addition, the methods of virus transmission from person to person are defined. Consequently, we should then be able to protect whomever is at high risk for death from this infection. We actually have now proven this with the shelter in place experience.

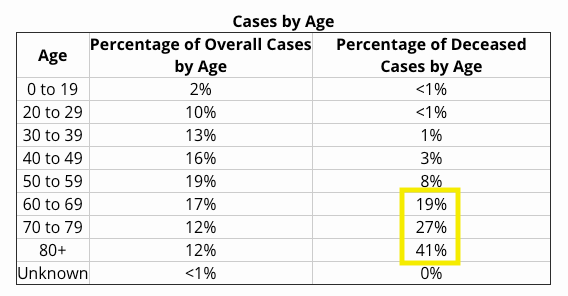
Given this knowledge we should be able to divide the country into two groups; those under 60 without health problems and those at risk for serious illness and death (everyone else). In order to release the first group of people to their routine activities without restrictions, we simply have to protect the latter group, which includes 94% or more of the deaths from COVID-19.
Therefore, these are the steps that I would recommend that allow us to normalize the country while at the same time preventing almost all of the excess death associated with COVID-19.
1) Release anyone under the age of 60 without a preexisting medical condition to totally normal activity. Do not screen anyone in this population for COVID unless they are symptomatic and require medical care, or they have a job that interfaces with the at-risk population.
2) Insist that social distancing, mask use, and other precautions continue for at-risk individuals over 60 and all those with medical issues.
3) Initiate emergency production and stockpiling of remdesivir and develop protocols for its early and immediate use in at-risk individuals.
4) Anyone over the age of 60 or anyone with a pre-existing medical condition must be seen by their physician and have blood pressure, heart disease, and diabetes management optimized before having restrictions eased.
5) Anyone who is still at medical risk must sign a waiver that they understand the risk if they normalize their activity.
6) Continue periodic screening (weekly would be optimal) for COVID-19 virus (not antibody) in healthcare workers and all other workers who come in contact with senior citizens. Those shedding virus are restricted from work for 14-21 days or until they have had two consecutive negative tests.
7) If by incredible good fortune a vaccine is developed, this vaccine should first be given to elderly and people at risk from the infection. Subsequently the rest of the population could be immunized to develop herd immunity and end the pandemic for good.
While using this approach would mean that some young people will still get sick and may even require hospitalization, this would not result in the type of tragedy we have seen with the massive deaths of elderly in our major cities. While this is a fairly simple proposal, it requires discipline and the ability to test at-risk individuals in a uniform and reasonable way.

I would like to forward to our Governer of Hawaii and Mayor here on Maui but I wonder if you didn’t mean to label the chart CASES by AGE. as from MICHIGAN and not S. KOREA??
LikeLiked by 1 person
I believe that’s how you cherry-pick data. Establish one story and switch to a different data set to prove your point.
LikeLike
The age-specific death rates risk over estimating the age effect and miss he heterogeneity in response. Seems to me that we need to know something about how rates of infection, symptomatic and unsymptomatic, vary by age before we institute broad age-based restrictions. Of course, chronic disease rates. increase with age, so age as you are suggesting can be used as a proxy for disease risk, but we’ll be able to make better judgments when we look at infection rates by age, and that will, of course, require broad testing.
LikeLike
Disagree. Look at the most recent Michigan numbers. The other confounding variables have disappeared. Age and medical problems are all that are left. We need to provide better care for everyone with health issues for sure, but essentially we can now define risk and use it for stratification of activity. And I fall in the high risk group.
LikeLike
There seems to be (in my circle of friends and friends of friends) some people finding out they have underlying conditions of which they did not know about, until being hit hard. How should we address this risk?
LikeLiked by 1 person
Go to the doctor and get them treated! A good wake up call!
LikeLiked by 1 person
Dear Dr. Baker, First, thank you for your intelligent, reasonable and informative blog. I look forward to it daily and am so grateful for your insights and wisdom. I’m a 75-year-old woman in good health, except for hypertension which is managed by meds. This sounds like a workable solution and I hope some of the decision makers take notice and consider your re-entry plan. Thank you for all of the time and energy you bring to this effort. Your humor provides a welcome relief as well. Gratefully, Kathleen Rogers
Sent from my iPad
>
LikeLiked by 1 person
I find this modest proposal very interesting. Is there any type of “task force” of professionals working on a plan? It would make sense to have a select group of your colleagues to establish “a plan”. As a medical professional myself, I do not want to hear from politicians. We need a sound plan driven my people like yourself.
And btw, I have really appreciated your blog. I share it daily with my friends on Facebook. Thank you. And stay well.
LikeLiked by 1 person
Yess, I agree that would make sense. I also think the “media” has done an incredible disservice to the country by magnifying issues that are not significant to scare up ratings. Need to have a true taskforce that directs and enforces scientifically sound policy.
LikeLike
Do we know anything about the effect of Obstructive Sleep Apnea and CPAP treatment upon Covid-19 mortality?
LikeLiked by 1 person
OSA is associated with metabolic syndrome , diabetes and cardiac issues. CPAP treatment is important to control those. If you use CPAP make sure your equipment is up to date and fits well. It will likely help. Remember, even with medical issues 80% of 80 year olds survive COVID!
LikeLike
This is very similar to what Sweden is doing isn’t it? Protect the sick and elderly and no restrictions for others.
On a different note, one critique I heard about our governor is that she is relying almost solely on medical advisors and not enough on people the from the business community. These medical advisors don’t seem to be leaning toward your method given that our stay at home continues to be extended. Assuming all doctors involved have good intentions and reasonable people can disagree, why do you think they are choosing a different path? One guess I have is they don’t trust the sick and elderly would stay home and thus would overwhelm the hospitals. Would love to know your thoughts on why we don’t see more medical people advocating for this.
Thank you for your blog!
LikeLike
I am not sure who is making these decisions in the state of Michigan. As a physician, I am confused by what the leadership in Lansing is telling me; there was an announcement today that the state’s chief medical officer wants us to provide needed services to patients but won’t let us open our clinics. Video won’t cut it for most services.
LikeLike
Hi Jim,
Your plan to reopen is excellent. I look at things very differently from you, and I am in quiet but rrspectful disagreement with many of your assessments and interpretations. But, in terms of reopenning America, we are on the same page.
Hoping you and your family are healthy and well!
Best wishes
Gus
LikeLike
Thanks Gus. I hope you’re well. I appreciate your input. Jim
LikeLike
I hope you share “your modest proposal” with “your friends in high places”. Well done.
LikeLiked by 1 person
If only I had friends…..
LikeLike
Eureka!
LikeLiked by 1 person
Your ‘modest proposal’ looks like exactly what we need to do now. The only issue is the over-60 folks who cannot afford to stop working and cannot work at home. Supporting these folks is a much smaller problem than our current one – maybe even two or three orders of magnitude. I’d just add lowering the age at which someone can start collecting Social Security to 60 or otherwise providing support.
LikeLiked by 1 person
I think we could be creative in jobs for these folks as well. Most of their skills don’t involve heavy lifting (literally) so working remotely or in restricted access would be a real possibility. After our current experience allowing this segment of the workforce to telecommute should not be a big issue.
LikeLike
With nearly three months of additional data since your proposal in May, how would you reevaluate your plan? Since there have been so many different approaches, which European countries and which American states do you think have been most successful in balancing health needs with business needs?
LikeLiked by 1 person