Three interesting articles came out concerning antibody testing in COVID-19. The first was a prepublication on antibody testing from Mount Sinai Hospital in New York City. The study was conducted from March 26 to April 10, 2020 and looked at 1,343 mildly symptomatic outpatient subjects (only 3% had been ill enough to be seen in the emergency department). The average age was 40 years, 91% were less than 60 years old and 53% were male.
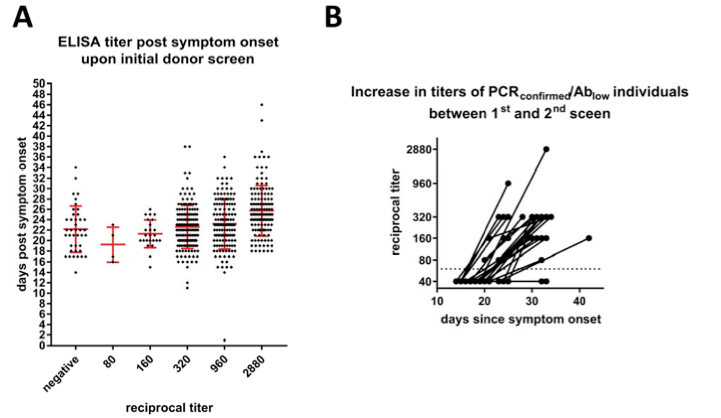
The study found that essentially all PCR-confirmed COVID-19 patients developed antibodies after being infected with COVID regardless of their symptoms. The antibodies were of high titer (strong) and increased over time (see figure).
This was important because many people were concerned that not all individuals would develop an immune response to the virus after infection, especially if they were asymptomatic. While I personally feel that no one recovers from this infection unless they have an effective immune response, it was good to see that patients with asymptomatic infection develop the same degree of immunity as those who had symptoms.
Of interest, this report also showed that in a large proportion of antibody positive individuals’ virus, genetic material can be detected via PCR in the upper respiratory tract for weeks post symptom resolution, but it was unclear if this signal represented infectious virus.
Two other studies showed results from large-scale antibody by screening of different populations. Both showed very low levels of antibody positive individuals that may be related to the unique populations they sampled.
First, major league baseball screened 26 of their 30 teams. Only 0.7% of major league baseball players and employees were positive for COVID antibody. This included both baseball players as well as club staff. Of those that had COVID-19 antibodies, 70% had no symptoms at the time they believed they were infected. This study was heavily biased towards athletes and club executives; 60% male and 80% white.
Another study involved screening random individuals in North Carolina, which is conducting the state’s first public study of coronavirus antibody prevalence. This study, from Wake Forest Baptist Health System, involved 676 individuals who voluntarily returned blood test kits (out of 1475 sent). The study’s lead investigator, Dr. John Sanders of Wake Forest University, reported that 2.2% of the participants were positive for COVID antibody. While this suggests a low number of people had been infected in the Research Triangle area, there was a selection bias in the returnees, which were predominantly white and female. This group, therefore, may not be representative of the area’s population.
Taken together, these last two studies suggest that the rates of COVID exposure (as defined by antibody) may vary widely across the country. Lower prevalence also may be related to whether individuals have the resources to facilitate their isolation/shelter in place.

Thank you for compiling this. It is quite interesting. Hopefully these high antibody levels will be found to provide many months of immunity, and this thing can go into hibernation while we await an effective vaccine.
LikeLiked by 1 person
Thank-you for an informative, scientific and logical assessment of the situation that can be understood by people with less scientific education than needed to process this mess. A friend at the university was very helpful and suggested your blog. So now I have to go read up on what a titer is and how it is used to present data…..
LikeLiked by 1 person