A third type of coronavirus test has recently been introduced. This test is somewhat like the swab or PCR test, because it directly looks for the presence of COVID-19. Rather than looking for viral RNA like the PCR assay, this test looks for viral proteins (antigens).
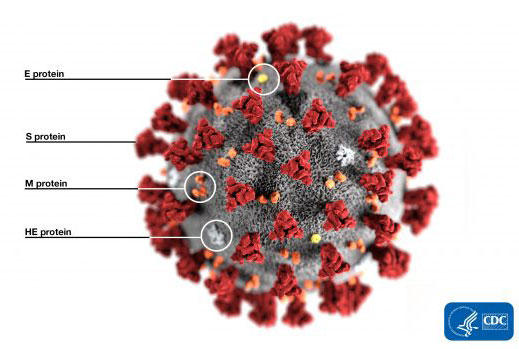

The antigen test as it is called involves the swab of the back of the throat, in a similar manner to the PCR test. But then the material is mixed together with antibody that binds to the antigen. This complex is then captured by another antibody. This allows the direct detection of the viral protein if the virus is present.
This approach has been touted as an advance in screening for the virus by Dr. Birx among others. Advantages to this approach include simplicity, because no complicated processing or large device is involved to detect this material. In addition, you can use a handheld device similar to an antibody test so that theoretically people can be screened almost anywhere within minutes. The need to screen potentially millions of people for virus would be much helped by this type of assay.
Unfortunately, these tests tend to be much less sensitive than PCR in looking for virus. The test identifies antigen without amplification in contrast to PCR. As a result, you can have a similar amount of RNA and viral antigen present on the swab, but the viral RNA will be amplified a billion times by PCR while the antigen is not amplified at all.
The approved antibody assays are required by the FDA to be 80% sensitive, which suggests that you’ll miss 20% of the people who are actually shedding virus. This is much lower than the 98% sensitivity rate seen with PCR using the same swab technique. Along with the lower sensitivity, the antigen test has all of the same problems as the PCR test in terms of throat sampling. Therefore, a combination of sampling variables and lack of amplification leads to a lower likelihood of detecting the virus.

Only one antigen assay has been approved by the FDA, and it is made by a company called Quidel. This essay claims to be close to 90% sensitive but requires a reader to identify the band associated with the antigen. This negates some of the benefit of having an antigen test since a device is involved. Also, there are reportedly only 36,000 readers distributed throughout the US. Despite this drawback, however, readings are done within 15 to 20 minutes so that rapid detection is achieved.
In summary, antigen tests may have some value in identifying people shedding the virus but are less sensitive than PCR assays and have the same problems around sampling of the upper throat using swabs.
