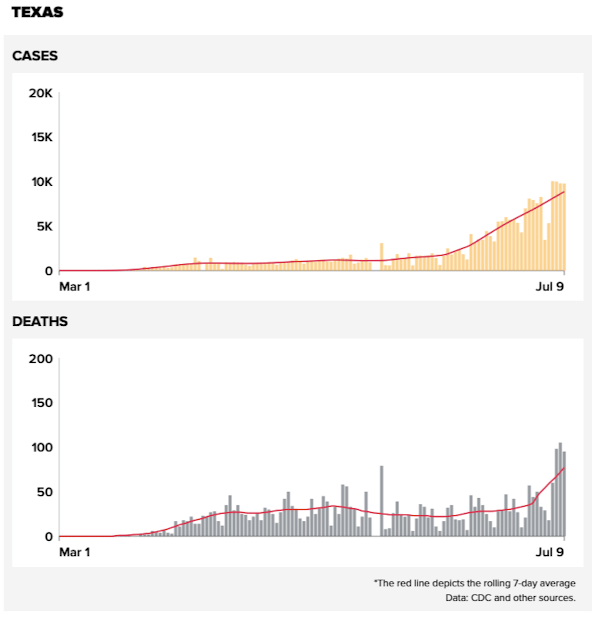
Houston is a new epicenter in COVID-19 infections. While the number of infections in Texas has been increasing progressively, those numbers have overwhelmingly come from a limited number of urban areas with Houston leading the way. There are a number of parallels between what is happening in Houston now and what happened in New York city three months ago; but there are also some significant differences. This is highlighted by two new reports from ProPublica.
Houston hospitals are being pushed in terms of occupancy. Much like New York City though, the need is particularly for intensive care unit (ICU) rooms as compared to regular hospital beds. If the experience in New York is any guide, the focus should be on creating additional ICU facilities given that the additional standard hospital beds (in field hospitals or hospital ships) were not needed or utilized.
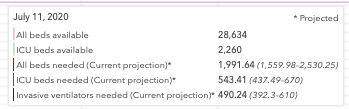
The biggest choke point in Houston again appears to be emergency rooms. Because of the lack of specialized hospital facilities, many patients are being kept in emergency rooms well beds are not available. This is not optimal because intensive care cannot be given in overwhelmed emergency rooms and this is generally associated with bad results for any disease. Importantly, the early care of COVID-19 patients also appears to be important in outcome of their disease.
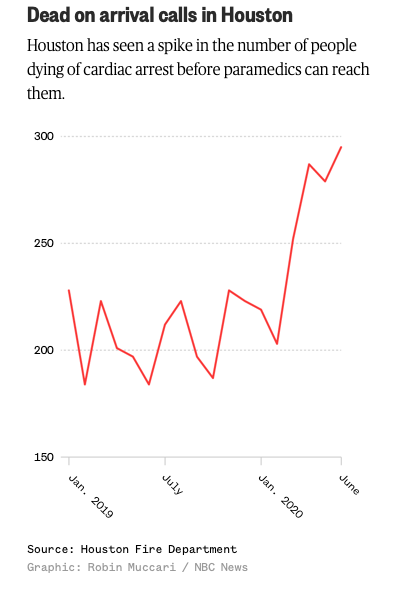
Also similar to New York, however, there clearly appears to be a reluctance to seek routine medical care in the middle of this pandemic. While this was also seen in Detroit and other early hotspots, it actually may be worse in Houston because individuals having observed the crises in other cities and are even less willing to go to the hospital during the COVID-19 flair in Houston. Another article by ProPublica has documented this leading to increasing numbers of deaths at home. In contrast, other stories have suggested that because there are no shutdown orders in Houston or Texas, there have been on going activities such as auto accidents that continued to stress hospital emergency services.
The most prominent difference in Houston has been that the death rate from COVID-19 has been lower in Houston than in earlier hotspots. Many reasons for this have been proffered including younger aged individuals being infected and better treatments. COVID-19 deaths in Houston are now starting to increase, and again many factors are potentially involved. It may be that home deaths are now being more accurately attributed to COVID-19, or that the care of individuals is deteriorated due to medication and ICU shortages. It may also be that infections in nursing facilities are now increasing, putting more vulnerable individuals at risk. Whatever the reason, the death rate must be watched.
In some ways it is reassuring that the COVID-19 outbreak in Houston looks very similar to earlier outbreaks in other cities. It suggests that the infection and the virus have not fundamentally changed. It also indicates that measures that were useful in controlling prior outbreaks will be effective in Houston and other cities, but only if they are expeditiously employed!

Thank you for your thoughtful posts on various aspects of this pandemic.
I’m concerned about all the people infected with Covid-19 who are not sick enough to warrant hospitalization, but sick enough to possibly have long term sequelae. Are there any guidelines for management or treatment of such cases?
On a related note: It seems that death and hospitalization are the primary indicators being tracked. There is also a lot of talk about asymptotic people. But there is a lot of territory in between. It seems hard to get a sense of the percent of the population that is disabled in other ways, a picture of the average course of the illness and typical outcome. What percent of people who test positive struggle with health issues weeks or months after the infection? Can you recommend a reference?
Many thanks,
Huda
LikeLiked by 1 person
Since the majority of people under 40 are asymptomatic this is an important issue. But there is no accurate reference for the outcomes. A few studies have suggested these individuals have lesser immune responses, but these studies use antibody assays that may be suspect.
LikeLike
One factor that it seems might contribute to fear of seeking more routine medical care is lack of testing. I would have expected that everyone who enters a hospital for any reason would be tested, and people who work there (medical or otherwise) would be tested weekly. Assuming the test results were available quickly, infected patients could be segregated from non-infected, and possibly health care workers as well. These protocols would protect people from getting infected at the hospital to some extent, and increase confidence that patients could safely seek treatment for non COVID-19 issues.
LikeLiked by 1 person