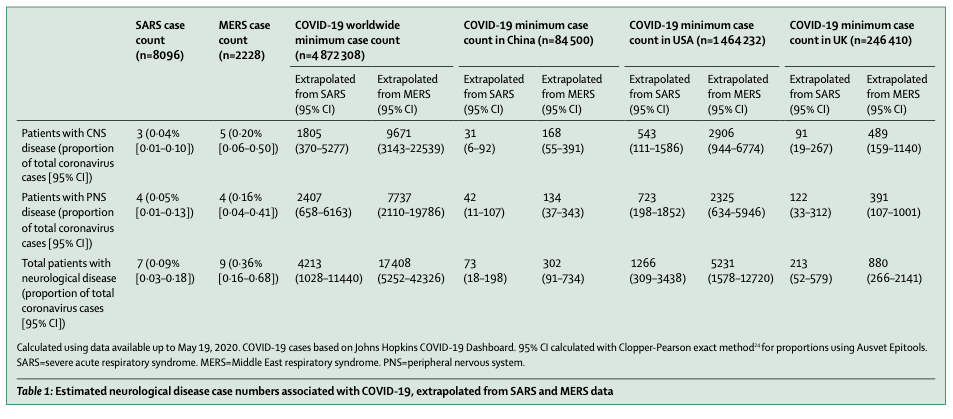
Over the past few days I’ve been concerned about several news stories focused on an exceptional number of severe neurological complications associated with COVID-19 infection. While these complications are not surprising, since almost every human viral infection is associated with some type of neurological disease, the spectrum of these complications was worse, and the implied frequencies seemed higher than might be expected. In particular, neurological problems with the pandemic coronavirus infection SARS were relatively infrequent (less than 0.1%).

In examining the publication that generated these news stories, I found that it was a review article in the journal Lancet. This review examined the published reports on COVID-19 looking for reports of clinical neurological abnormalities. This paper is therefore a “review of reviews.” It did not look at specific patients that the investigators identified, but simply interpreted the reports of others on COVID-19 neurological disease.
The investigators found a relatively small number of patients (901) with neurological disease associated with COVID-19 in the entire world’s literature. Also, while there was a wide array of neurological manifestations in these 901 patients, the authors admitted that “many had insufficient detail to evaluate” and this reflects “the challenge of studying such patients.“
They concluded that “careful clinical, diagnostic, and epidemiological studies are needed to help define the manifestations and burden of neurological disease caused by SARS-CoV-2. Precise case definitions must be used to distinguish non-specific complications of severe disease (eg, hypoxic encephalopathy and critical care neuropathy) from those caused directly or indirectly by the virus, including infectious, para-infectious, and post-infectious encephalitis, hyper-coagulable states leading to stroke, and acute neuropathies such as Guillain-Barré syndrome.”
In other words, it was difficult (impossible?) to know if COVID-19 infection was the cause of these neurological problems.
In some ways, this report seemed to be at odds with other clinical publications highlighting COVID-19 manifestations. For example, acute cerebrovascular disease (stroke) is reported as an important complication, with studies reporting it in 2–6% of patients hospitalized with COVID-19. However, they found only 96 patients with stroke in the literature.
In contrast, despite not being identified by any of these lay publications, a much more coherent publication on COVID-19 neurological disease came out in the lesser-known journal Lancet Neurology. This publication actually did look at patients, in fact all hospitalizations for Covidien in the UK from this April 2 to April 26 of this year. They identified 153 individuals out of all the thousands of COVID-19 patients admitted to hospitals (not just infected) during these three weeks that met the criteria for neurological-psychiatric disease a frequency of neurological complications much lower than was predicted from the extrapolations from SARS.
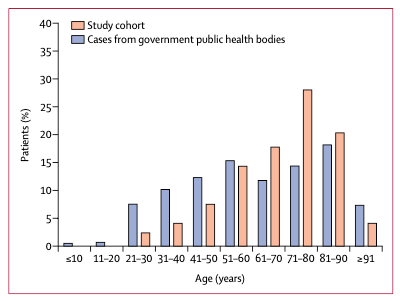
Most patients with neurological conditions were older than 60, the peak being older than 70. While half had cerebrovascular disease, a third had only altered mental status which could be due to almost any cause.
Therefore, while serious neurological complications do exist with COVID-19 and can be directly related to infection with the virus, they are rare. Particularly, some of the more complex neurological diseases, such as Guillain-Barre syndrome are very rare with this infection. Stroke is the most common problem but may be related to underlying vascular disease in these elderly patients.
