One of my most intelligent friends asked me today why we never talk about the treatment of COVID-19. My sad reply was that we still have no really effective treatments for SARS-CoV-2 infection.
Current research still has not identified who is at risk for severe COVID-19. While advanced age and other risk factors such as obesity, diabetes, and high blood pressure have been identified, most people with those risk factors do not get ill. This means we cannot identify and give prophylactic therapy to most people to prevent illness from COVID-19; we have to treat people after the infection happens.

Unfortunately, after 18 months of pandemic we have made only minimal progress in treating those people who are seriously ill with SARS-CoV-2 infection to improve their survival. The only antiviral drug that has been shown to be of any value, remdesivir, is of marginal benefit and must be given very early in the infection.

Monoclonal antibodies have shown some utility against the infection, especially in patients who have immune problems. But antibodies cannot stop the infection once it’s started. Monoclonal antibodies also appeared to be ineffective with variant viruses that are unique from the original strains of COVID-19 and able to escape binding by the monoclonals.
The biggest advance in treatment for COVID-19 involves the use of steroids. These drugs have been effective in suppressing inflammation associated with SARS-CoV-2 infection in the lung. This has improved outcomes in patients when started early enough in COVID-19 pneumonia.
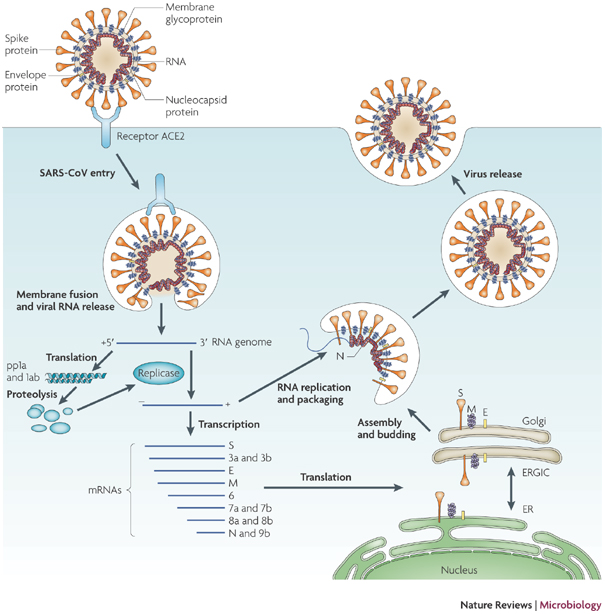
Why have COVID -19 antiviral drugs been difficult to develop? Viruses are unique in that they usurp normal cellular mechanisms to replicate. Therefore, drugs that block viral replication also tend to block normal cellular events. This makes it hard to develop drugs that stop viruses because they often have toxic effects on normal cells.
The SARS-CoV-2 virus that causes COVID-19 is relatively simple and has fewer unique activities that can be targeted than a more complex virus like HIV (AIDS). One of the reasons we now have effective therapy for HIV is that drugs were developed for several independent viral activities and used in combination. Like SARS-CoV-2, any single antiviral drug was minimally effective, but the combination of three, uniquely functioning antiviral drugs makes HIV a treatable disease.
Recently, the Biden administration announced that they will start a $3.2 billion-dollar initiative to try to develop antiviral drugs against COVID-19. Called “The antiviral program for pandemics,” the program is administered through NIH: “… partnering NIH institutes and centers initiated a robust research program to prioritize and accelerate development of COVID-19 therapeutics.” Projects will be “led and overseen by NIAID, NIH’s National Center for Advancing Translational Sciences, NIH’s Office of Research Infrastructure Programs, and the Biomedical Advanced Research and Development Authority, part of the HHS Office of the Assistant Secretary for Preparedness and Response.”
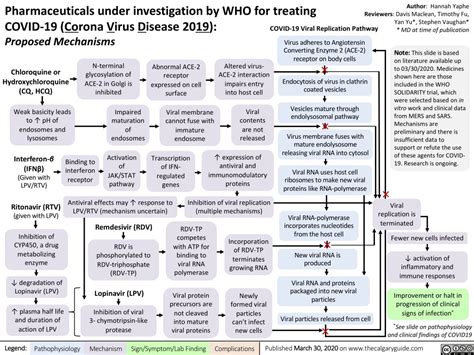
This is a noble pursuit, but top-down research rarely achieves results in medicine. Many of the top-down initiatives in the Trump administration that try to re purpose anti-malarial and anti-rheumatoid arthritis drugs were not successful.
The best way to try to develop new drugs for COVID-19 is to learn more about how the virus works. The more we know about the intricacies of how the virus infects and replicates itself in human cells, the more likely it will be that we will identify crucial points that can block the virus. We also will find opportunities where viral activities differ from normal cellular metabolism that could be specifically inactivated.
Hopefully, we will at some future time have effective therapies for COVID-19. In the meantime, we are remarkably lucky to have effective vaccines that can prevent this disease. People should take advantage of these vaccines and not wait for a drug.
