Pfizer has announced they plan on asking FDA for emergency use approval for a booster COVID-19 vaccine shot. This request seems to be related more to Pfizer’s revenue stream than to any acute need for a booster. There is no evidence of a failure of the Pfizer-BioNTech vaccine efficacy against any of the variant viruses, including the “Delta variant” which is now prominent in most of the world. Also no apparent drop off in immunity over time has been identified yet.
While I suppose it’s good that they are thinking ahead to a time, likely far away, when we potentially will need a booster shot, the noise related to this new topic unfortunately just seems to confuse individuals who are on the fence about getting the current vaccines. It would seem to be more important to focus on having everyone over 12 years of age in the U.S. and around the world immunized with two doses, preferably with one of the mRNA vaccines.
The second piece of information is somewhat more disconcerting. The Johnson & Johnson vaccine was associated with Guillain-Barré syndrome. This is an autoimmune, nervous disorder that can cause paralysis, but was rare occurring in only 1 of 125,000 doses given. It was seen mostly in men over the age of 50, and almost everyone who got Guillain-Barré reportedly recovered.

This latest autoimmune problem with the Johnson & Johnson vaccine, which was previously associated with a rare autoimmune blood clotting disorder, shows the issues that can be expected with a more complex, adenovirus-based vaccine. The more proteins present in the vaccine, the more likely the vaccine will cause the immune system to attack normal human proteins and result in autoimmune disease.
The J&J vaccine has 38 proteins from adenovirus, along with the single, COVID spike protein required for COVID-19 immunity (the only protein made by the mRNA vaccines). Importantly, these other viral proteins are irrelevant to inducing immunity to COVID-19 since they are not related to that virus. I attach my prior blog post on the adenovirus-based vaccines which explains in more detail the autoimmune potential of these vaccines.
The advantages of the Johnson & Johnson vaccine supposedly were single dose administration, ease of manufacturing, lower cost, and thermal stability. Manufacturing has been a nightmare in the U.S. due to the problems at Emergent, Johnson & Johnson’s manufacturing partner, and the other benefits have not been significant for the United States or most developed countries. While there may still be some benefit for the Johnson & Johnson vaccine in areas where the RNA vaccines aren’t available, its use in the United States will likely be very limited.
Prior Blog Post: The real difference in adenovirus based COVID-19 vaccines.
Now that the Johnson & Johnson adenovirus based COVID-19 vaccine has been approved again for use in the U.S., I think it’s important to provide perspective to individuals who are considering taking this vaccine. My comments also pertain to any of the adenovirus based COVID-19 vaccines, including the AstraZeneca and the Russian vaccines.
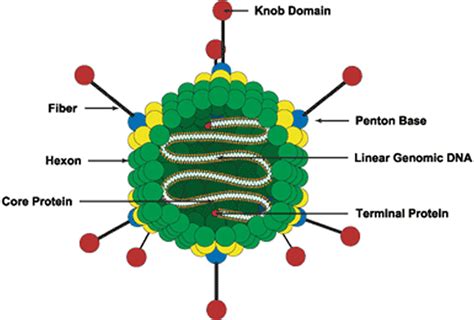
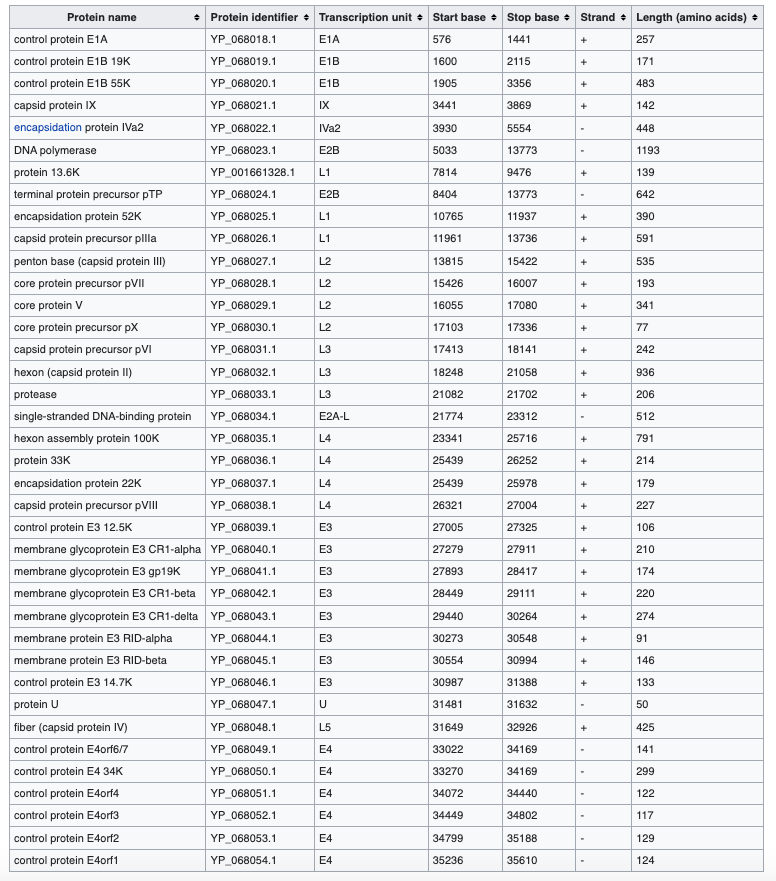
As reported in Wikipedia, Adenoviruses (members of the family Adenoviridae) are complex viruses. The name of the virus derives from their initial isolation from human adenoids in 1953.[2] They contain at least 38 proteins.
There are more than 50 distinct human adenoviruses (serotypes) that cause a wide range of human illnesses, from mild respiratory infections in young children (the common cold) to life-threatening multi-organ disease in people with a weakened immune system.[1]
These viruses have a 20-sided capsule (covering) strongly protecting their genetic material (nucleocapsid). The genetic material itself is double stranded DNA genome, which is very stable and similar in structure to human genes. In addition, because these viruses have no outside lipid covering, they are not easily degraded by heat or detergent. Adenoviruses are the largest known non-enveloped viruses.
The stability of adenoviruses is a large part of the attraction to using them as the basis for vaccines, since storage and refrigeration are less onerous. Also, methods of genetically modifying and manufacturing adenovirus are well developed.
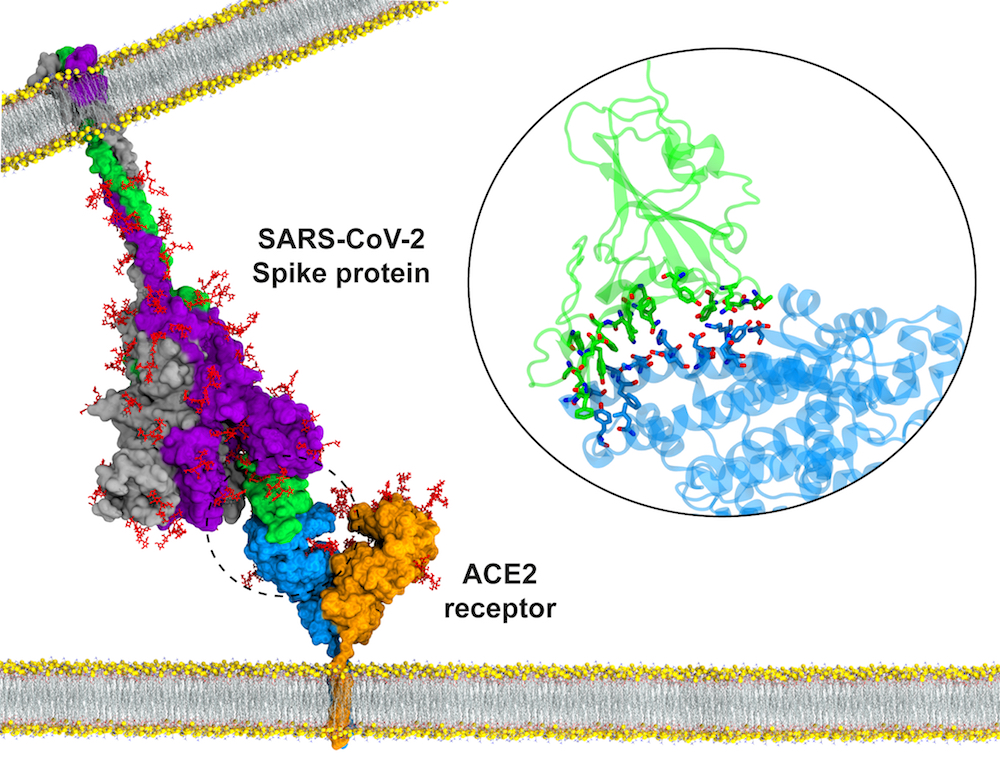
In contrast, SARS-CoV-2, the virus causing COVID-19, is a slightly smaller virus with a lipid envelope and unstable, single-stranded RNA as its genetic material. While it has 29 proteins, only one, the spike protein, is necessary to induce protective immunity. In fact, the RNA vaccines (Pfizer-NBioTech, Moderna) produce only a fragment of the spike protein and result in highly effective immune protection.
Why do I think it is a problem to use whole adenovirus to immunize against COVID-19?
It is not because it will cause adenovirus illnesses. When used in vaccines, the adenoviruses are modified in a way that prevents them from reproducing in humans. Thus, while these viruses can still infect humans, in vaccines they do not cause infection related disease.
My major concern is the need to inject 38 different adenovirus proteins and adenovirus double stranded DNA into an individual to induce immunity to a single fragment of an unrelated SARS-CoV-2 protein (that has been added to the adenovirus). The person being injected with this vaccine will make immune responses to all 38 adenovirus proteins along with the important fragment of the SARS-CoV-2 spike protein.
Because adenovirus infections are so common, almost every person has already been infected with adenovirus by the age of 18. Therefore when an individual receives an adenovirus based vaccine, it is a booster response to the 38 adenovirus proteins. This results in intense immunity to the adenovirus proteins, often even stronger than the immunity generated to the coronavirus spike protein included in the virus!
Making an immune response to all of these different viral proteins could lead to an immune response to your own proteins (that look like the viral proteins). This could cause your immune system to attack itself resulting in autoimmune disease. This was only a theoretical concern until the blood clotting issues arose and appeared to be related to autoantibodies to platelet factor 4, proving that this concern was real.
Why is this rare autoimmune disease only seen in young women? For reasons that are not entirely understood, young women are more prone to autoimmune disease, and this likely is related to hormones. Not surprising, this predilection decreases after menopause sparing older women. Also, the rarity of the autoimmune disease is likely because it only happens in individuals that have certain genes in their immune systems that cause them to develop these cross-reactive antibodies.
In any case, injecting a whole, unrelated virus with 38 proteins to induce immunity to a single fragment of SARS-CoV-2 spike protein does not seem an optimal vaccine approach, especially compared to the RNA vaccines which induce immunity only to the spike protein.
Regardless of this, we do need to have everyone vaccinated against COVID-19.
If you have no option but the Johnson & Johnson vaccine because you live in an area where you cannot obtain one of the RNA vaccines, then by all means get vaccinated with that vaccine. The risks are rare. However, if you have the option, and especially if you’re a woman of childbearing age, try to get one of the RNA vaccines.

Is there anything to Israel data implying Pfizer efficacy starts fading after six months?
LikeLike
see today’s post.
LikeLike