There has been much argument about the origin of the virus that causes COVID-19. Concerns have focused on the potential that this virus was engineered by scientists in China or was in some way an accidental release of natural virus by the Wuhan Institute laboratory. The initial source of SARS-CoV-2 has yet to be identified, but the complexity of this virus is so great that it seems to challenge the concept of “human engineering.”
Human evolution of this virus is happening however and is the result of the infection of unvaccinated individuals. This evolution occurs as the virus infects and reproduces itself inside of people. All the while the SARS-CoV-2 virus is mutating to become more dangerous.
A recent paper in Science magazine details the SARS-CoV-2 evolution resulting from the infection of millions of unvaccinated people. Those infections serve as the perfect engineering platform to make this virus worse.

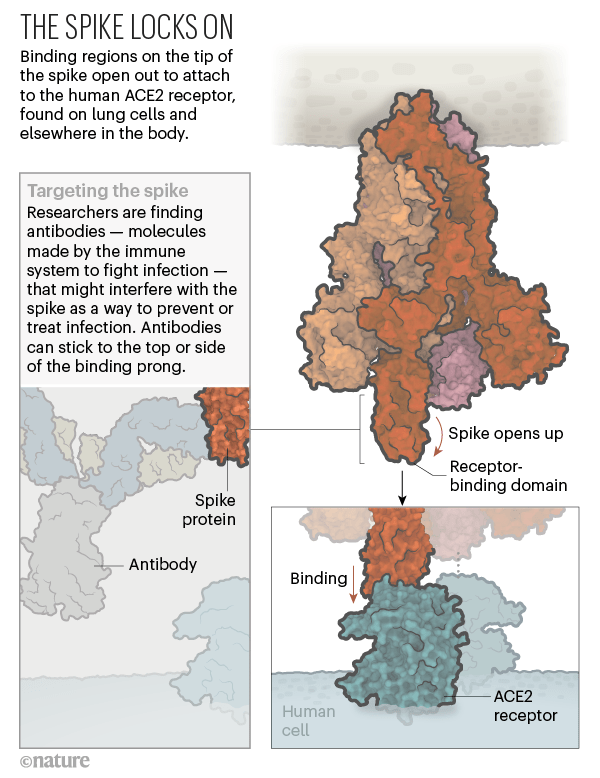
This paper examined the spike protein on the surface of the virus that mediates its binding to human cells. They found specific and unique changes in the protein that would have been hard to anticipate and that resulted in a more infectious virus that in some cases could outwit antibodies.
The SARS-CoV-2 variants this group studied had multiple spike mutations that enable increased infectivity in humans and the potential to resist immunity. This study used electron microscopy and assays that measured the binding to human cells.
Not surprising, all variants that evolved in humans showed increased angiotensin-converting enzyme 2 (ACE2) receptor binding that improved the ability to infect people.
Much of this improvement came from an increased propensity for receptor binding domain (RBD) fragment of the spike protein to be in its active, extended or “up” state. This is the area that specifically binds to the ACE2 protein on human cells.

Once the virus becomes more infectious it can start to resist developing immunity in unvaccinated individuals. This was documented in the UK (B.1.1.7) variant spike protein which balanced stabilizing mutations (that improved infectivity) with destabilizing mutations (that help evade immunity). A destabilizing effect on the spike protein structure caused by another single amino acid substitution in the Brazil and South Africa virus variants (RBD E484K mutation) also led to resistance to neutralizing antibodies.

The only way to stop this evolution is to get everyone in the world vaccinated to SARS-CoV-2. This kills the virus before it has a chance to mutate and prevents the virus from using your body as a laboratory to improve itself!

One thing I’m not understanding is the notion that only the vaccines provide effective immunity to SARS-CoV-2; that natural immunity from being infected and having COVID-19 is less effective than a vaccine. It seems to me that with natural post-COVID-19 immunity there would be antibodies produced against a number of viral components and not just the spike protein. Wouldn’t this target more phases of the viral infection than the single binding protein found in the spike? If you would please clarify this for me I’d surely appreciate it!
LikeLiked by 1 person
The biggest issue is the booster shot. Having another dose of antigen to help establish memory immunity is important. That is why most suggest at least one dose of vaccine after natural infections.
LikeLike
As the vaccine was developed to the original less infectious and resistant strain, is the original vaccine going to be sufficiently effective against the new strains?
That we are seeing infections in vaccinated people suggests the vaccine needs to be modified to meet the new viral mutations.
LikeLike
Cellular immunity will provide protection even with antibody escape. Think this is why even breakthrough infections don’t result in serious disease.
Best,
Jim
LikeLike
Fair.. But I only chose two of among many reports. Hopefully it doesn’t get buried for polical reasons. To me, anecdotal is more realistic than oftentimes flawed studies.
LikeLiked by 1 person
I am less worried about politics than incompetence. CDC wasn’t even following breakthrough infections. Need to continue to monitor especially with so man unvaccinated spreading the infection.
LikeLike
What to make of this latest buzz? : Dr. Kobi Haviv,(the medical director of Israel’s leading center for respiratory care) via Channel 13 said An Israeli doctor says that the majority of COVID-19 patients hospitalized and the ones with the most severe illness at his hospital (Herzog Med Ctr) are fully vaccinated. 85-90% and 95% respectively.
He also claims one infected patient will spread the virus to “a large number of people, happening frequently.
LikeLike
Needs to be put in context. Compared to a year ago, (July 28, 2020) Israel diagnosed 2,125 total new cases of the virus, compared to 2,267 that were diagnosed on Wednesday. However, on July 28 last year, there were 320 serious cases, whereas on Wednesday there were only 149. So total number of infections are down significantly with vaccination.
This hospital is in an area where literally everyone in the hospital has been vaccinated, but includes may immunocompromised individuals and those with other illnesses. Another doctor pointed out that one of his hospital’s serious patients is an 87-year-old who has been on a respirator for three months, meaning he is not even from the current wave. He then added “the Delta variant is very infectious, but infection among those vaccinated is much less severe. When the numbers rise, we see an exception here or there, like the young pregnant woman who was vaccinated and ended up with severe disease and on a respirator. But I believe she will recover much easier than patients like her during the third wave.”
So statements like Dr. Haviv’s need to be carefully examined. Clearly there are reasons why some who have been vaccinated would get infected, but the overall infection rate with vaccines is still 8 fold lower than in the unvaccinated.
LikeLike
P.S.: I also see from the recent outbreak of COVID-19 in eastern Massachusetts that a whopping 87% of the cases of breakthrough infections are in men. Over the course of the pandemic those of us who’ve paid attention have noted that men are much more susceptable to this virus than are women (presumably due to their more numerous ACE-2 receptor sites.), but now it looks like the vaccine is far less effective for men than women as well. The authors note that the events where the infection spread was marketed mainly to men, but that doesn’t really reflect the demographics of actual atrendees. Presumably lots of men bring their wives, daughters, female companions, et.al., to these events on Cape Cod and the nearby islands in Barnstable county. Any thoughts on that?
https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w#contribAff
LikeLike
These events were targeted exclusively towards gay men with few women in attendance. Hence the sexual distribution.
LikeLike
Do you worry that the administration of vaccines of mixed efficacy is leading to evolution of stronger variants? Since the vaccines don’t prevent infection but only severe disease, it seems that this practice allows the virus to infect and continue to evolve in more hosts. Similar to the concept of overuse of antibiotics leading to antibiotic-resistant bacteria, it seems like overapplication of vaccines that aren’t fully neutralizing the virus, will lead to worse versions of the virus over time?
LikeLike
This is a theoretical concern, but compared to the viral replication and variant potential of the unvaccinated, it is minor. I have at several times suggested we make enough RNA vaccines for the entire world!
LikeLiked by 1 person