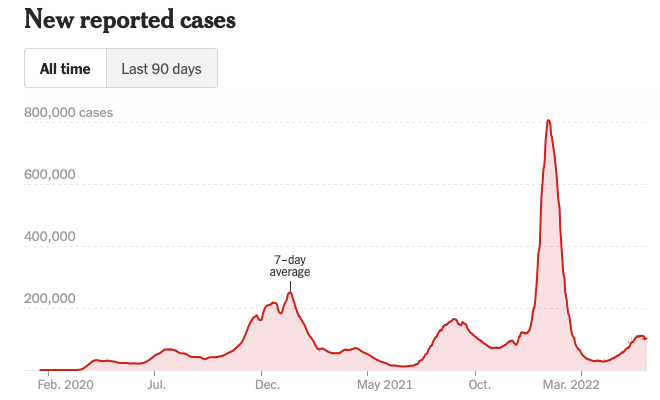
As the latest wave of infections from COVID-19 winds down, the strongest indication that the fundamental dynamic of this pandemic has changed has been the stark drop in virus-associated deaths.
The daily average of deaths from COVID-19 now stands at 264, which is a 12% drop in the 14-day average over the prior two weeks. In addition, the hospitalizations and ICU admissions have also dropped in the last two weeks. Infections in “hotspots” like Michigan also have dropped significantly since May.
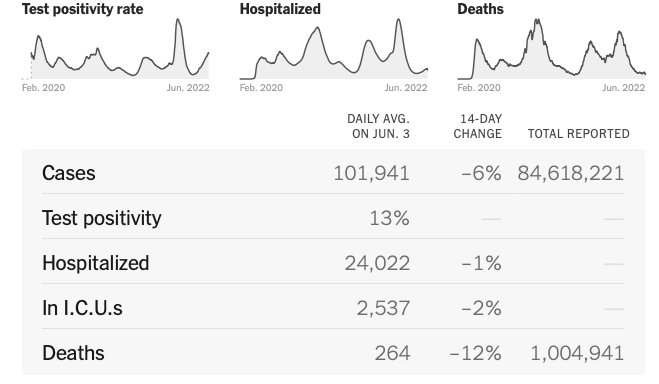
These changes need to be understood in the current dynamic of reporting hospitalized COVID patients. There are significant government incentives for health care systems to screen and diagnose patients with COVID-19. In response, hospitals are now more often diagnosing patients admitted for other illnesses. Therefore, someone admitted for a broken leg and incidentally found to have COVID-19 is counted as if there were a hospital admission for COVID-19.
Thankfully, the decreases in serious illnesses and deaths from COVID-19 are being seen despite stalled immunizations against SARS-COV-2. Despite calls for additional boosters, rates of immunization in the U.S. are not increasing. As I have indicated before, however, the current rounds of infection are acting like additional vaccinations that will eventually protect the population against these coronaviruses.
Almost immediately, media attention has turned to rare reports of monkeypox infections as a new concern. I have not commented on monkeypox, but some of these statements that have recently been made have inspired me to speak up.

Monkeypox is very different from COVID! First, it is not transmitted by respiratory mechanisms. It infects skin and mucous membranes and therefore requires direct physical contact to spread. This makes it much more limited in its ability to infect populations and unlikely to cause a pandemic.
Importantly, monkeypox is caused by a very different type of virus. Poxviruses are double stranded DNA viruses and do not mutate quickly like coronaviruses that are based on a single strand of RNA. This means monkeypox does not rapidly generate virus variants so there should be no concern that it will escape immunity or cause different types of disease. In fact, the vaccine against the most serious form of poxvirus, smallpox, provides nearly lifelong immunity against infection.
Poxviruses can cause serious disease, and having personally seen disseminated smallpox in HIV infected, immune deficient individuals who had received the live smallpox vaccine, I know it certainly is not something to be taken lightly. On the other hand, some poxvirus diseases are fairly mild, and this includes molluscum contagiosum which causes a wart-like rash in (predominantly) adolescent swimmers and wrestlers. Monkeypox illness is somewhere between these extremes.
The current outbreak of monkeypox appears to be related to a few large gatherings of individuals who had significant physical contact with each other. These events were similar to the event in Provincetown, MA that led to a spread of COVID, but the current situation resulted in many fewer monkeypox infections. Importantly, the gatherings included individuals who came from areas where monkeypox is endemic, so it is not surprising the infection was spread.
Therefore, if you don’t participate in these large gatherings, you should not be worried about being infected with monkeypox! End of story.
