One of the most frightening aspects of coronavirus (COVID-19) infections is that people in the prime of their lives are dying acutely without any definable medical problem. While these deaths are infrequent compared to the number of elderly people with heart and lung disease who are dying from COVID-19, they appear to be fundamentally different in their cause. Understanding this difference is crucial to learning how to treat this disease.
Elderly people with heart and lung disease have minimal tolerance for any type of stress to their system. The infection further deteriorates marginal lung and heart function and leads to respiratory and heart failure. People with these illnesses are prone to die from any respiratory infection, whether it is flu, a bacterial pneumonia, or coronavirus. Most of the people who die from influenza, much like COVID-19, fall in this group.
In contrast, young people who die from COVID-19 infections have a very different illness. They seem to get acutely ill and develop a systemic attack on many of their organs. While these patients can also die from respiratory failure, there is no predisposing illness. They often have failure of the other organs. This is been ascribed to an acute inflammatory response, now being called “cytokine storm.”

Cytokines are the hormones produced by the body as part of the immediate response to an infection and cause the immediate signs of infection, like a fever. This immediate response is called “innate immunity,” because the response is hard wired into every human and is similar for any type of infection (virus vs. bacteria). Innate immunity’s job is to alert your body to the fact that there is an infection and wake up the immune system to respond.
The innate immune response is produced by cells like macrophages and neutrophils. These “white blood cells” respond non-specifically to infection and produce innate inflammation in the lung. Normally, after the innate inflammatory response, the immune system makes a specific response to the virus that neutralizes it and kills the virally infected cells. This is how you clear the body of a virus infection and heal your organs.
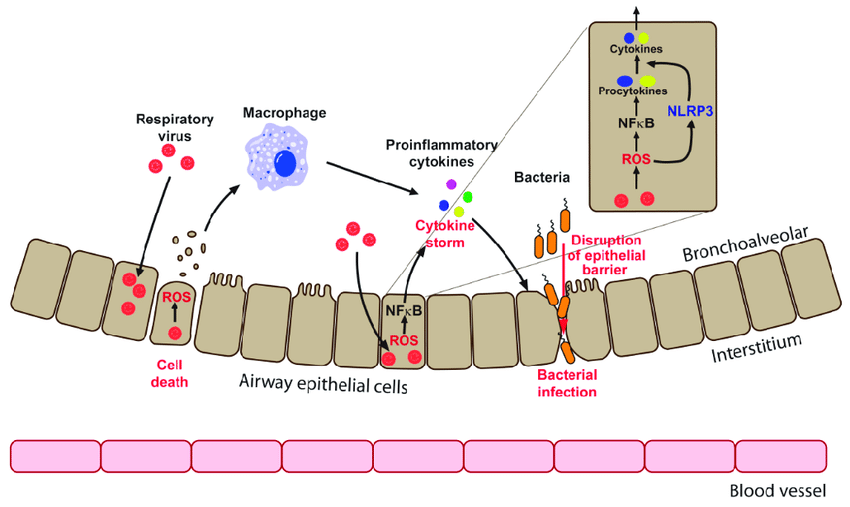
People who die from acute coronavirus infection seem to have an exaggerated innate response and a delayed specific response, so that they fail to clear the virus. The body continues to flail at COVID-19 with inflammation in an attempt to wake up the immune system. However, this causes organ damage and can lead to death.
Why does this happen? We now know that several hundred genes control each individual’s immune response. Remarkably, these genes are highly variable among different individuals. This is purposeful. By having a variety of different immune systems, the human race can better handle different types of infections. This, in turn, assures that some percentage of the human populace survives almost any type of infection. Supporting this hypothesis, populations that are genetically similar tend to have massive numbers of deaths with certain infections (see measles in the Hawaiian islands).

Young people who acutely die from COVID-19 should have specific variations in the genes controlling their immune response that put them at risk for coronavirus. We should immediately start saving genetic material from every young person who dies from COVID-19 infection. We now have the ability to sequence (examine) every single gene that controls the immune response, and we could identify variations in these genes called polymorphisms. We can define the polymorphisms that alter the control of innate immunity that predispose individuals to die from COVID-19 infection. This was useful with SARS and should be more valuable with COVID-19, given the acute death rate.

Understanding genetic predispositions to death from COVID-19 will allow us to identify “markers” that put people at risk from this infection. Importantly this information will also provide insights into potential therapies. Currently, several companies are testing drugs that will suppress innate inflammation in a general way to attempt to address this problem. Having specific, genetic targets for drugs could be a huge improvement on this approach.
We will be proposing that we undertake studies like this at the University of Michigan and hope that universities across the country join in this effort.

Thanks for the update. I will keep drinking my fresh ginger tea daily. I’ve discovered it helps with the inflammation from arthritis, so I hope it precludes other inflammations.
LikeLike
Is there any over the counter anti-inflammatory that might be helpful in blunting the body’s immune response?
LikeLike
some are trying steroids, but others think they worsen lung disease. No benefit from NSAIDS.
LikeLike
very interesting thank you
LikeLiked by 1 person
Jim. Thank you for crushing it with these thoughtful and informative posts. You are providing information not easily found elsewhere.
LikeLiked by 1 person
Jim: I am trying to keep up, but going back just 3 or 4 days you were discussing sub-clinical infection. I have two questions: 1. People ask when will this be over? Based on what you know now, how would you answer this question? and 2. When the first wave of this virus ends and we look back on it, how will the five categories you have described be divided? The five are people who never experienced the virus, sub-clinical infection, infection, hospitalized illness and death.
Thank you. randy
LikeLiked by 1 person
Think the peak is mid April through May. See https://covid19.healthdata.org/projections
Think you have the categories exactly right.
Best,
Jim
LikeLike
Boomer another great post. But where is that photo from–all the patients side by side in an armory or some place?
LikeLiked by 1 person
Fascinated by the article on cytokines. With 40 plus years in Internal Medicine working for the State Dept overseas, I saw several young healthy persons who unexplicately died. This
LikeLiked by 1 person
Wow. Thank you for this… Glad to have stumbled upon your page!
LikeLiked by 1 person